
Anyone can choose to donate their blood and save many lives. Well... almost anyone.

Illustration by Kallum Best
Choosing to donate blood is an incredibly altruistic and rewarding act. You are deciding to literally give away part of yourself, often to a stranger, to improve their quality of life or perhaps even save it. But in many parts of the world, men who have sex with men (MSM) are not even offered this choice. This is because certain countries place sweeping and stringent restrictions on males who have ever engaged in sexual relations with other men. These are sometimes called ‘deferrals’, perhaps to soften the blow. But calling it that doesn't take away from the fact these are limiting and, in some cases, unfair policies.
For instance, MSM are not allowed to donate blood or blood components in a staggering number of developed and developing countries. This long list includes several European countries including Germany, France and Denmark and spans across the globe to very populous places such as Hong Kong. Until recently, this was the case in Australia, too, but after nearly three decades of indefinite deferrals, the standard policy changed nation-wide by 2000. Now MSM donors can donate if 12 months have passed since the last sexual encounter.
Other developed countries followed suit and by 2016 the United States, Canada and the UK had all instated 12-month deferrals. There are also a small number of countries with shorter wait times, such as New Zealand and South Africa, which require a five and six-month wait, respectively. Interestingly, there are countries that don't have any specific restrictions or waiting periods in place at all. In Spain, Italy and Russia, the need for a deferral is based on how risky the donor’s sexual history is. All in all, it is a rather mixed bag, which raises the question: why are these deferrals in place at all?

The current global policies on blood donation from men who have sex with men, as of 29 January 2017. The deferral policies range from no deferral (light green), no deferral except for blood transfusions (fluorescent green), temporary deferral (yellow) and permanent deferral (red). Rtheranikal/Wikimedia Commons (CC BY-SA 4.0)
How and why these policies came into existence
Back in the 1970s, the patterns of transmission of the human immunodeficiency virus (HIV) were not understood. For many years, there were numerous isolated cases across the globe of individuals dying from a confluence of infections. It was not yet known that this mysterious disease, which would later be named acquired immune deficiency syndrome (AIDS), was caused by HIV and transmitted through infected bodily fluids including blood.
By the 1980s, many thousands of people who had received blood transfusions had become infected through HIV-positive blood, which had been donated by unwitting carriers of the virus. Globally, blood supplies were compromised. There was no test to detect the presence of HIV. The only evident link was the high prevalence of AIDS in the MSM community and the inkling that this may be a blood-borne disease. Blood service providers and blood banks decided to deal with this emerging pandemic by imposing permanent bans on male donors who had engaged in oral or anal sex with men.

A microscopic look at the blood shows the red blood cells that carry oxygen around our body, and the T cells (orange) and platelets (green) that play other important roles. Zeiss Microscopy/Flickr (CC BY-NC-ND 2.0)
Evolution of testing procedures
Over the next two decades, there was an advent of scientific knowledge surrounding this virulent disease and development of diagnostic procedures for its detection in blood. The western blot and enzyme-linked immunosorbent assay (ELISA) were the first such tests to be used due to high sensitivity in recognising specific antibodies, the immune molecules that the human body produces in response to infectious agents. As it turned out, these tests were sensitive to only one sub-type of HIV (only HIV-1, not HIV-2). There was also the issue of the ‘window period’, which is the period of time during which someone who has contracted a virus can still test negative for it. In the case of these particular tests, this was three to six months. There was a fear that these ‘false negative’ tests would allow infected blood to enter the donor pool. As a result, blood service providers decided to keep the indefinite deferrals in place.
Newer methods were steadily developed and the accuracy of tests kept increasing, with the leap to nucleic acid testing (NAT) coming a decade and a half after the indefinite restrictions were first implemented. This test was much more sensitive and drastically reduced the window period to just 12 days. More recently, an even more sensitive test called the chemiluminescent immunoassay (ChLIA) was developed. It is able to detect antibodies for both subtypes of HIV, unlike the earlier tests. The new tests also have the ability to detect a host of other transfusion-transmissible infections, such as hepatitis B virus (HBV), hepatitis C virus (HCV), syphilis and human T-lymphotropic virus (HTLV). Despite these apparent advances in testing techniques, unlimited deferrals have persisted in many countries, much to the chagrin of the MSM community.

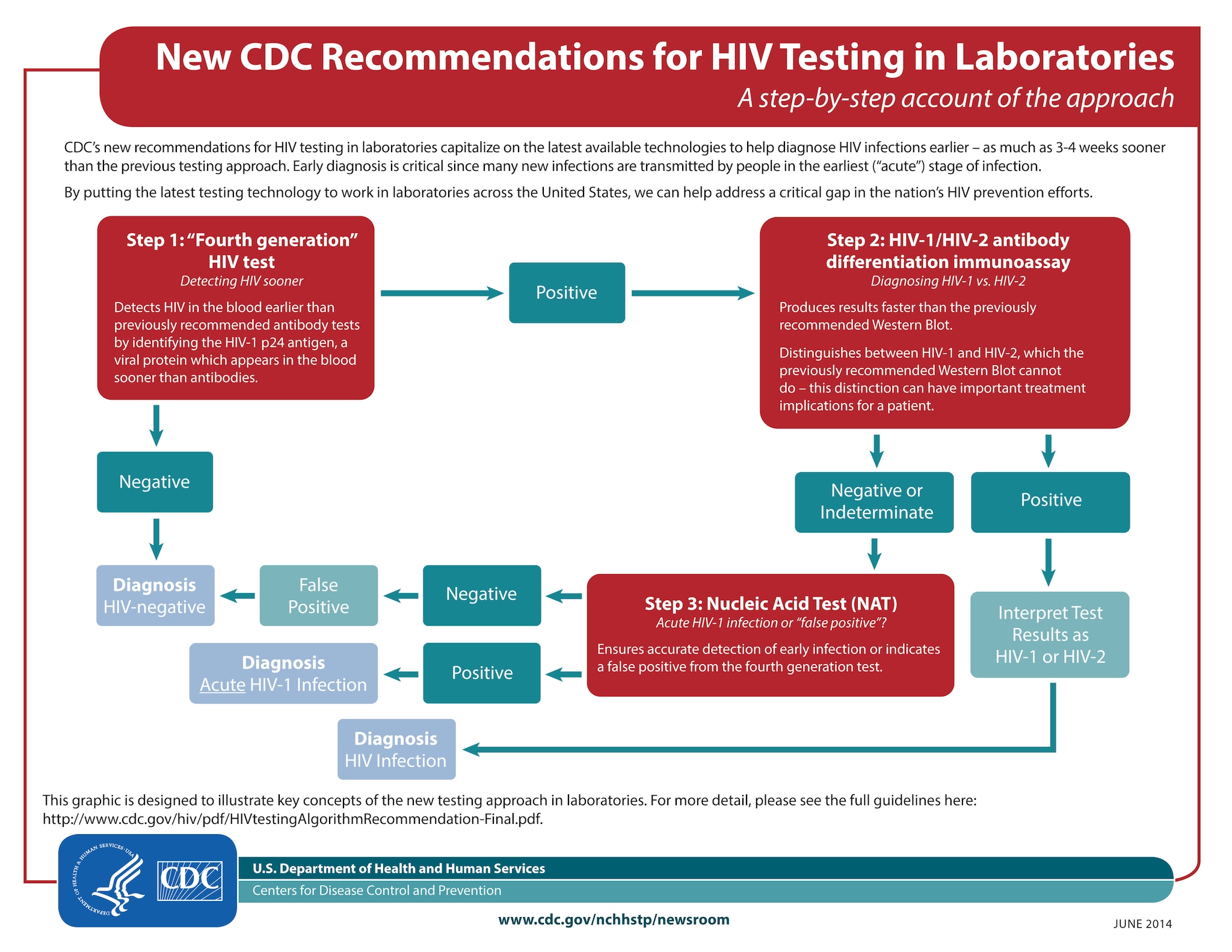
The Centers for Disease Control and Prevention outlined their recommendations for HIV testing in this flowchart from 2014, encouraging the use of new technologies that enable diagnosis three to four weeks earlier. Centers for Disease Control and Prevention.
Let’s talk about sex...
One of the main reasons that MSM are more likely to contract and spread sexually transmitted infections (STIs) such as HIV comes down to basic biology. The cells lining the openings of our anatomical back doors are much thinner than those lining the vagina so they are more susceptible to tears. To add to this, semen and this cellular lining can carry, and hence transmit, more of the virus than vaginal fluid. Anal sex is also much more common among MSM, and there is a higher chance of condoms tearing than during vaginal sex, compromising their intended protective effect.
The most recent statistics (2016 Annual Surveillance Report) surrounding STIs don’t help the situation. The Kirby Institute, which has studied trends in infectious diseases for decades, found that even though HIV infection rates had stabilised, there were still a significant number of new HIV diagnoses made. Nearly 70% of these were attributed to sexual contact between men. There has also been a steady increase among MSM in the number of cases of other transfusion-transmittable infections (TTIs), including syphilis and Hepatitis B.
Contemporary research that changed things
While it may seem that these facts and figures portend a rather bleak outlook, there is still hope. In 2012 a landmark study, authorised by the Australian Red Cross Blood Service (ARCBS), reviewed the existing 12-month deferral policy. A call was put out to the public to glean what they felt about these deferrals and a panel of experts was approached for their recommendations. Based on this, the ARCBS then went on to conduct further research to determine how compliant or truthful donors were being when questioned about their sexual activity on donor screening questionnaires. All these investigations found that there was no tangible risk of TTIs being spread through blood transfusion from MSM donors given the current blood testing techniques and donor screening methods. They concluded that reducing the deferral time to six months would not endanger our blood supply. Armed with this information, the ARCBS appealed to their regulatory body, the Therapeutic Goods Association, in 2014. However, the proposal was not successful. Incredibly, this research formed the groundwork for other countries’ decisions to relax their deferral policies. There have also been initiatives such as the Rainbow Donor Clinic, started by the Canadian Blood Service, aimed at encouraging MSM donors to give blood, which can be used for research and testing purposes.

Perhaps more countries will soon move to shorten deferral times for blood donations by men who have sex with men. Bart Maguire/Flickr (CC BY-NC-ND 2.0)
What’s in store next?
Even though progress has been made, these changes may be too incremental and slow for many people. Given that the bans still require abstinence for the stipulated period of time, this may just put people off donating even after the deferral period ends. This means missing out on a significant number of donors, some of whom may have rare blood groups for which there is a dire need, particularly with ever-changing population dynamics in countries like Australia. It is absolutely imperative that our blood supplies are kept safe and adequately stocked. If changes are to be made to deferral periods, these ought to be evidence-based and the evidence points to shorter wait times. Regulatory bodies may not be willing to remove the deferrals and it may not be practical for blood services to tailor their questions to assess each potential MSM donor based on their individual sexual history. Indeed, the ARCBS review found that reducing the deferral period to three months seems to be the most scientifically sound middle ground, as this would even cover the window period for HCV.
Hopefully, ongoing research will help bolster the case of blood service providers such as the ARCBS. There are also concerted efforts from advocacy groups like the Australian Federation of AIDS Organisations that are hoping to reduce these restrictions. Until then, given that this is a contentious issue, change may be slow. All we can do is wait and hope that the power of sound science wins.
Disclaimer: This article reflects the personal views of the author and not those of any previous or current employers.
Edited by Ena Music.





























































{kind=link}
{kind=link}